1262
Views & Citations262
Likes & Shares
Objective: To
determine the contribution of CT in the etiological diagnosis of seizures in
adults in sub-Saharan Africa.
Patients and
Methods: A descriptive retrospective study of a period of twelve months that
concerned all patients older than 15 years, in whom was performed a brain
computed tomography (CT) for seizures. This study was performed in the
radiology department at the University Hospital of Yopougon (Abidjan, Ivory
Coast).
Results: The
mean age of patients was 42.9 years with extremes ranging from 15 years to 77
years. The sex ratio was 2. Fever was the sign most frequently associated with
seizures (23.8%) followed by the post critical coma (19.8%). CT scans were
pathological in more than half of the cases (57.1%). The predominant
pathologies were meningoencephalitis (20.7%) followed by the
cortico-subcortical atrophy (16.7%) and extradural hematoma (16.7%).
Conclusion: Cranioencephalic
CT scan showed its diagnostic efficacy in over half of the cases in the
assessment of seizures in Abidjan. The etiologies found were dominated by
infectious cerebrospinal meningitis pathology. MRI should be popularized in
sub-Saharan Africa to go further in this etiological research.
Keywords:
Seizures, Cranioencephalic CT scan, Stroke, Brain abscess
INTRODUCTION
Seizures
in adults are a common clinical situation. In France, they represent 0.3 to
1.2% of the reasons of admission [3-6]
to the emergency unit and the risk in the general population to have seizures
is estimated at 5% [3-7]. In the
Ivory Coast, they represent 8% of admissions to the intensive care unit
according to the studies of BOUH et al. [8].
The
diagnostic approach in the presence of seizures in adults is based on a full
examination interview, a thorough clinical examination and well oriented
additional tests. Medical imaging is an integral part of the diagnostic
strategy. It plays a key role. It is represented by computed tomography (CT)
and magnetic resonance imaging (MRI). In our African context, apart from
epileptic seizures, seizures in adults are a common reason for cerebral CT
request. When we know that this examination has a significant cost, it is
legitimate to wonder about its real contribution in the etiological research of
seizures in adults. The aim of our study was to determine the contribution of
CT in the etiological diagnosis of seizures in adults (epilepsy excluded).
Patients and Methods
It concerned all patients in whom it was performed a brain computed
tomography (CT) for seizures. This study was carried out in the radiology
department at the University Hospital of Yopougon in Northern Abidjan in a
popular area called Port-bouet II. Were included, all patients with a complete
CT account mentioning (gender, indications, technique of performance and
detailed results) and whose age was above 15 years. CT scans were performed on
a Toshiba scanner apparatus with 64 bars. A cranioencephalic acquisition in
spontaneous contrast was performed with or without another acquisition after
injection of iodinated contrast medium according to the case. The parameters
studied were age, gender, technical protocol and the results of CT.
RESULTS
All of our results are
detailed in Tables 1, 2 and 3.
Forty-two CT scans were
performed on the grounds of seizures in adults out of a total of six
hundred Cranioencephalic CT scans
performed during the study period. This represents an incidence of 7%. The
percentage of male subjects is the largest in 66.7% of patients with a sex
ratio of 2. There was a predominance of patients aged 25-34 and those aged
55-64 in 23.8% of cases. The average age was 42.9 years with extremes ranging
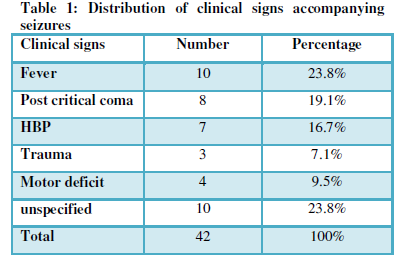
from 15 to 77 years. Fever was the clinical sign accompanying seizures more
frequently (23.8%) followed by critical post coma (19.8%). In 76.2% of cases,
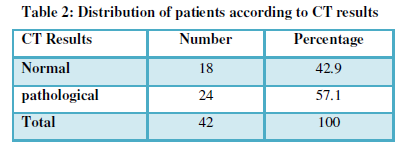
CT scans were performed with injection of iodinated contrast medium. CT scans
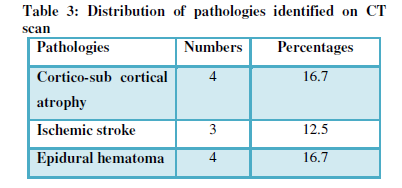
were pathological in more than half of the cases (57.1%). The predominant
pathologies were meningoencephalitis (20.7%) followed by the cortico-subcortical
atrophy (16.7%) and extradural hematoma (16.7%). The other diseases were tumors
(12.5%), stroke (12.5%), leukoaraiosis (12.5%), brain abscess (4.2%) and
hydrocephalus (4.2%). These different pathologies can be classified into 5
groups that are in decreasing order of frequency: vascular pathology (25%),
infectious disease (24.9%), disease sequelae (20.9%), traumatic pathology
(16,7%) and tumor disease (12.5%).
DISCUSSION
We performed a
Cranioencephalic scanner to all our patients with in 76.2% iodinated contrast
medium injection against 24.8% in spontaneous contrast. We agree with the
American College of Emergency Medicine [7]
that recommends a cranioencephalic scanner for all patients admitted to the
emergency department with a first seizure. But the CT protocol depends on the
etiology that underlies the occurrence of seizures. It is therefore right that
Wilden et al. [8] believe that all
cranioencephalic scanners to explore seizures should be first performed without
iodinated contrast medium injection in order to exclude fatal bleeding injuries
that may require an urgent neurosurgery intervention. Then, according to
Sempere et al. [9], another
acquisition should also be performed after injection of iodinated contrast
medium in HIV infected patients or patients with a history of cancer in order
to exclude an abscess or tumor.
In our study, CT scans were
pathological in more than half of the cases (57.1%). Our results differ from
those of Sudhir [10], in India, in
which only 24% of patients had normal exploration. This difference can be
explained by the fact that the study of Sudhir included both scanners, MRI,
biological analyzes and EEG while our study was based only on CT. According
Esquevin [11], the scanner is
limited for the research of hippocampal anomalies, a tumor lesion of small size
or malformation. In all cases, a brain CT scan interpreted as normal does not
dispense with the performance of brain MRI.
The pathologies that we
highlighted in the CT exploration of seizures were dominated by
meningoencephalitis (20.7%). According Bouh et al. [8], causes of seizures seem to be influenced by the geographical
origin or level of development, with a predominance of infectious and vascular
causes in sub-Saharan Africa, while in the Western countries alcoholic and drug
causes seem more important. Indeed, Mbodj [12]
in his work on the management of convulsive status epilepticus in developing
countries has found a prevalence of infectious causes (67%). In America,
alcohol is among the top three causes of status epilepticus (39%), followed by
drug toxicity (14%).
According to some authors [9-14] etiologies can be classified
according to age. For these authors, we must distinguish the causes of
convulsive seizures in young adults from those in the elderly. In the northern
countries, causes of seizures in young adults are dominated by toxic causes
(alcoholism, drug intoxication, poisoning energy drinks, etc ...). Lee et al. [13] described in 2015, a case of
convulsive seizures in a subject younger than 36 years, a chronic alcoholic
with vitamin B6 deficiency. Unlike younger subjects, all Caucasian authors
describe tumor and vascular causes, with a predominance of tumor pathology, in
subjects over 60 years [9-14]. In
our study, these vascular causes were represented by ischemic stroke and high
blood pressure materialized on CT scans by leukoaraiosis lesions. Hemorrhagic
strokes were not visualized in our series. If that classification by age should
be admitted in sub-Saharan Africa, the causes of seizures in young patients
would be dominated by infectious causes and those in the elderly would be
dominated by vascular pathology. Indeed, in the study by Ongolo et al. [14] on seizures related to Toxoplasma
meningoencephalitis, subjects were aged 24, 36, 38, 46 and 58 years. No patient
was older than 60 years. In the study of Goita et al. [15] in Mali, that concerned a series of 26 patients, the mean age
was 38.1 years, with extremes ranging from 18 to 56 years. Other etiologies
such as sequelae pathologies and traumatic pathologies were found in our study.
Neishige [16] in Japan reported several
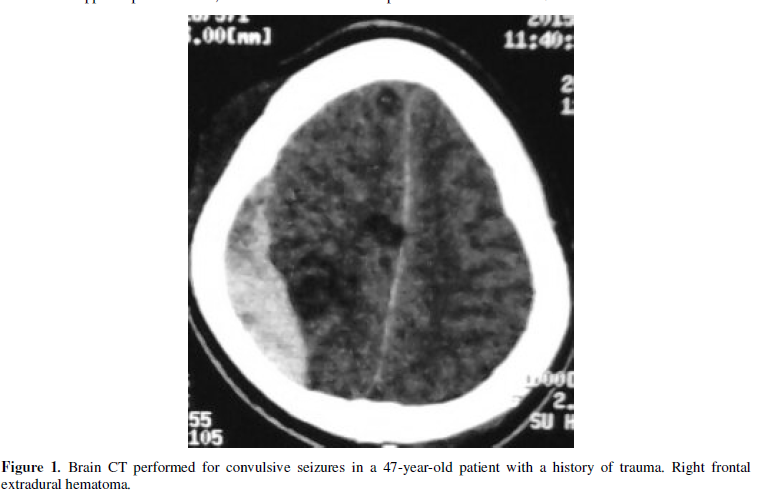
cases of subdural hematoma as a cause of seizures. In our study it is rather extradural
hematoma. We agree with Duffour et al. [17]
who described a case of seizures in connection with an extradural hematoma of
vertex in a 36-year-old woman. Sequelae pathologies encountered in our study
were brain atrophies and one case of hydrocephalus. Chaudhary et al. [18] reported a case of seizures
responsible for hydrocephalus. Metabolic causes of seizures and alcoholic
poisoning have not been found in our study. Unlike Bouh et al. [8] who showed metabolic causes in
13.7% of cases. This could be explained by the fact that our study did not
include biological data.
CONCLUSION
Convulsive seizures are
rarely explored in a radiology department. They represented 7% of reasons for
the performance of cranioencephalic scanner. They affected predominantly men
and were accompanied by fever in most cases. Cranioencephalic scanner that is
to be performed mostly without and after contrast injection showed its
diagnostic efficacy in more than half of the cases. The etiologies found were
dominated by vascular pathology in the elderly followed by infectious diseases
in young subjects unlike studies carried out in Western countries where toxic
causes are predominant in young subjects and tumor causes in the elderly. Given
our results, MRI exploration and a toxicological assessment associated with a
well conducted interview should complement the scanner that should keep its
place in an emergency unit.
CONFLICT OF INTEREST
None.
1.
Huff JS,
Morris DL, Kothari RU, Gibbs MA (2001) Emergency
department management of patients with seizures: a muticenter study. Acad Emerg Med 8: 622-628
2.
Bhatt H,
Matharu MS, Henderson K., Greenwood R (2005) An
audit of first seizure presenting to an accident and emergency department. Seizure 14: 58-61
3.
Dunn
MJG, Breen DP, Davenport RJ, Gary AJ (2005) Early
management of adults with an uncomplicated first generalised seizure. Emerg Med J 22: 237-42
4.
Smith
PE, Cossburn MD (2004) Seizures: assessment and
management in the emergency unit. Clin Med 4:
118-122
5.
Jallon
P, Loiseau P, Loiseau J (2001) Newly diagnosed unprovoked
epileptic seizures: Presentation at Diagnosis in CAROLE study. Epilepsia 42: 464-475
6.
Bouh KJ,
Ayé YD, Babo C, Konan KJ, Yeo TLP, et al. (2014) Aspects épidémiologiques des
états de mal convulsif en réanimation au chu de Yopougon. Rev int sc méd 2: 110-113.
7.
ACEP Clinical Policies Committee,
Clinical Policies Subcommittee on Seizures (2004) Clinical policy: critical
issues in the evaluation and management of adult patients presenting to the
emergency department with seizures. Ann
Emerg Med 43: 605-625.
8.
Wilden JA, Cohen-Gadol AA (2012) Evaluation of First Nonfebrile Seizures. American Family Physician 86: 334-41
9.
Sempere AP, Villaverde FJ,
Martinez-Menéndez B, Cabeza C, Peña P, et al. (1992) First seizure in adults: a
prospective study from the emergency department. Acta Neurol Scand 86: 134-138.
10. Sudhir U, Kumar AT, Srinivasan G, Kumar RV, Punith K (2013) Aetiology of seizures in elderly. J
Indian Med Assoc 111: 686-688
11. Esquevin A, Carsin-Nicol B, Mineur G, Aguilar-Garcia J,
Nica A, et al. (2014) Imagerie de la
première crise convulsive de l’adulte. Société Francaise de neuro-radiologie.
12. Mbodj I, N’diaye M, Sene F,
Salif Sow P, Sow HP, et al. (2000) Prise
en charge de l’état de mal épileptique dans les conditions de pays en
développement: les états de mal épileptiques périodiques. Clinical Neurology
30: 165-169.
13.
Lee DG, Lee Y, Shin H, Kang K,
Park JM, et al. (2015) Seizures Related
to Vitamin B6 Deficiency in Adults. J Epilepsy Res 5: 23-24.
14. Ongolo-Zogo P, Mbede M, Kouanfack C, Njamnshi AK (2013) Aspects Diagnostiques et
Evolutifs de l’Encéphalite Toxoplasmique chez le Patient VIH Positif. Health Sci Dis 14: 1-4
15. Goïta D, Karambe M, Dembélé JP, Sogoba D, Sidibé AF, et
al. (2012) Toxoplasmose cérébrale au cours du sida dans le service des maladies
infectieuses du CHU du point-G, Bamako-mali. Mali Médical 2012 Tome XXVII
1 : 47-50
16.
Neshige S, Sekihara Y, Ishii N,
Sato M, Ota S, et al. (2014) Clinical
and radiological studies of seizure in chronic subdural hematoma--case control
study. Rinsho Shinkeigaku 54: 869-875.
17.
Dufour H, Métellus P, Manera L,
Fuentes S, Do L, et al. (2001) Spontaneous
vertex extradural hematoma: considerations about causes. Case report and review
of the literature. J Neurosurg
94: 633-636.
18.
Chaudhary N, Mahato SK, Khan S,
Pathak S, Bhatia BD (2015) Neurocysticercosis
(NCC) with Hydrocephalus, Optic Atrophy and Vision Loss: A Rare Presentation.
J Clin Diagn Res 9: 1-3.
-
 Table 1
Table 1 -
Table 2
-
Table 3
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)


